
Key Points:
- Age-associated factors, such as systemic inflammation and an altered gut bacterial composition, can impede the balance between muscle protein synthesis and breakdown, leading to muscle loss.
- Along with exercise and a nutritious diet, supplementation may help improve muscle function and physical performance in individuals of advanced age.
- Supplements under review for enhancing muscle function in elderly adults include protein, L-carnitine, vitamin D, magnesium, potassium, and caffeine.
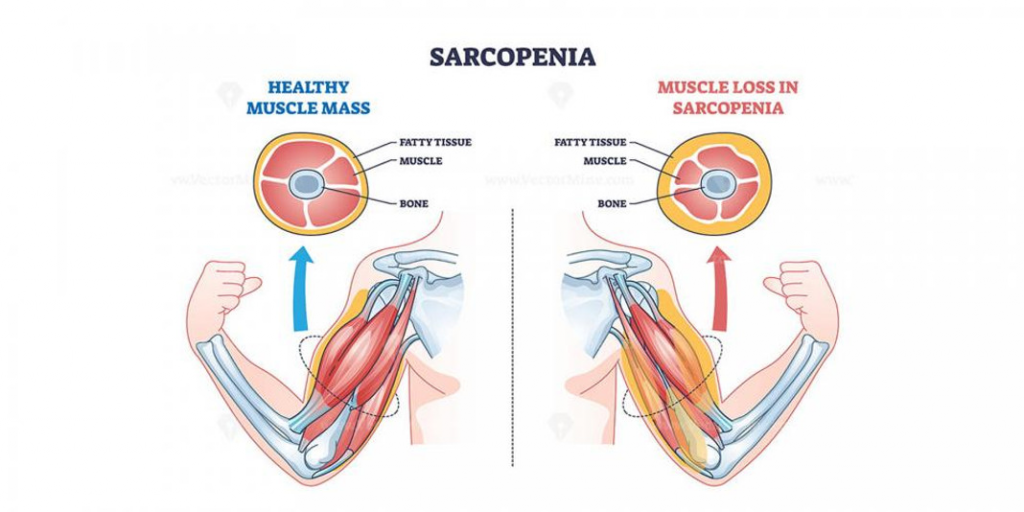
Whether taking supplements can support muscle function and physical performance as people age has garnered the attention of Walker and colleagues from University College London, as published in a review in Nutrients. Delving into their research on certain supplements can help uncover which, if any, supplements may aid older adults’ efforts to support their physical capacity. Relatedly, the data presented on supplements may also give important insight into preserving muscle function, since somewhere between 10% and 20% of older adults develop age-related sarcopenia, where muscles lose mass, strength, and function.
A Balance Between Muscle Protein Synthesis and Breakdown During Youthful Years
Fully functional skeletal muscles (which move the limbs and other parts of the body), typically exhibited during youthful years, allow the performance of activities of daily living, such as mobility, maintaining posture, and breathing. During younger ages, this type of muscle is a highly plastic tissue, meaning that it can grow (hypertrophy) and decline (atrophy) in response to a range of stimuli.
To maintain muscle mass and strength, a balance between muscle protein synthesis and breakdown is tightly regulated. In that regard, the rate of muscle protein synthesis is driven primarily by the consumption of food, dietary protein intake, and physical activity.
Along these lines, a key hormone involved in muscle protein synthesis is insulin, a hormone that the pancreas releases in response to eating. Insulin allows the sugar, glucose, into cells and also stimulates muscle hypertrophy, mediated by the secretion of another hormone called insulin growth factor 1.
In contrast to the mechanisms behind muscle hypertrophy, those involved in muscle protein breakdown include stressors like illness, a lack of physical activity, and inflammation. As such, an imbalance where muscle protein breakdown exceeds muscle protein synthesis leads to a loss of skeletal muscle, in physical states like aging-associated sarcopenia. It follows that this kind of musculature dysregulation can strongly impact insulin sensitivity, glucose levels, and metabolism, potentially facilitating metabolic dysfunction. Importantly, nutrients are essential for the mechanisms behind muscle function and help regulate the balance between muscle protein synthesis and breakdown.
How Getting Older Takes a Toll on Muscle Function
As people get older, muscles become less responsive to normal signaling that typically induces muscle protein synthesis. For example, older people can have lower insulin sensitivity, which makes their muscles less responsive to insulin. This blunted responsiveness explains, in part, the progressive decline in skeletal muscle mass, strength, and physical performance with advanced age. Moreover, this deteriorating skeletal muscle function can hinder people’s abilities to carry out daily tasks, like self-care, dressing, moving around, and eating.
Notably, muscle mass starts to decline as early as age 30 and is estimated to decline precipitously by 1% to 2% each year from the age of 50 onward. Critically, this age-related, excessive loss of skeletal muscle leads to sarcopenia.
Combining Exercise with Supplements May Support Muscle Function and Physical Performance During Aging
Walker and colleagues’ review examines research suggesting that combining regular exercise with certain supplements may help preserve muscle function and physical performance with age. Taking a closer look at the data behind these supplements, along with consulting with a doctor, can help individuals decide whether they may want to take them in an effort to stave off muscle deterioration and sarcopenia associated with advanced age.
Protein
Protein is an essential component of muscles and numerous aspects of physiological function, and protein supplementation has become popular among athletes and aging individuals. Accordingly, older individuals use protein supplementation to promote muscle growth and repair following bouts of exercise.
As far as dosage goes, a consensus recommendation for sedentary individuals is an average daily intake of 0.8 g/kg of body weight. Thus, for an average US adult weighing about 76 kg (about 168 pounds), the recommended daily dose of protein would be around 61 g.
All the same, some researchers believe that older adults may benefit from larger daily protein quantities, estimated at around 1.2 g/kg of body weight. As such, an average older adult weighing 76 kg may attain benefits from consuming about 91 g of protein daily.
The rationale for older people requiring more protein relates to their natural loss of muscle mass during aging, which can progress to sarcopenia. In that regard, the combination of a high-protein diet with resistance exercise has been found to mitigate sarcopenia in older adults.
Moreover, there is some evidence that protein supplementation may reduce the risk of bone fractures in post-menopausal women with osteoporosis. Furthermore, research has shown associations between protein supplementation, increased bone mineral density, slowed bone loss, and reduced hip fracture risk. Additional research has uncovered protein supplementation’s association with other longevity-related benefits—a lack of impairments in physical function and memory, good mental health, and not having a major chronic disease, like diabetes or multiple sclerosis—in a study of 3,721 nurses.

As such, research on protein supplementation seems to support its popularity among the aging population. Targeting muscle growth and repair with protein supplementation in the elderly may serve as a key method to prevent or slow age-related sarcopenia.
Creatine
Creatine is a compound made up of three amino acids (glycine, L-arginine, and L-methionine) that has essential roles in energy metabolism, energy storage, and muscle contraction. Interestingly, creatine is used to rapidly regenerate cellular energy in the form of the molecules ATP and ADP when there is a high energy demand. As such, creatine helps provide a quick source of energy for activities like high-intensity exercise.
Creatine is one of the most widely used supplements, and in addition to getting an estimated 1 g to 2 g of creatine daily from dietary sources, creatine supplementation is recommended at 0.1 g/kg of body weight daily. This means that for an average adult weighing 76 kg, the recommended dose would be about 7.6 g daily.

In older adults, supplementation with creatine in addition to a resistance exercise routine has been found to increase muscle mass and strength, not to mention improve physical function for activities of daily living. Other research has demonstrated similar results in aged patients with sarcopenia. At the same time, creatine supplementation without exercise was found to be mostly ineffective. Altogether, with evidence suggesting that creatine supplementation (in addition to maintaining a consistent exercise regimen) can improve muscle mass and function, choosing to take creatine may serve as a way to preserve physical performance with age and potentially delay sarcopenia.
β-Hydroxy-β-Methylbutyrate (HMB)
HMB is a metabolite of the amino acid leucine and is present naturally in animals as well as humans. Importantly, two forms of HMB have been studied: calcium HMB (HMB-Ca) and a free acid form of HMB (HMB-FA). Supplementing with either form of HMB appears to be safe in humans for at least one year with no negative effects on glucose levels or insulin sensitivity. Along those lines, recommended doses range from 1 g to 3 g daily for adults.

HMB’s primary action on muscles appears to be the enhancement of muscle protein synthesis and inhibition of muscle protein breakdown. As such, HMB is believed to facilitate muscle growth and repair, reduce muscle damage after exercise, and promote muscle recovery, especially when consumed around the time of physical activity. Furthermore, additional benefits from HMB supplementation may include increased lean muscle mass and reduced fat mass. Thus, supplementing with HMB in addition to exercising may help slow or counteract age-related sarcopenia and frailty.
L-Carnitine
L-carnitine is an amino acid derivative that plays a critical role in the body’s energy production. As such, it helps transport fatty acids into the cells’ powerhouses (mitochondria), where the fatty acids are utilized to make cellular energy in the form of ATP molecules.
Efficient use of fatty acids to produce ATP in muscles is tied to lower production of harmful, oxygen-containing molecules called reactive oxygen species (ROS). Therefore, sufficient cellular levels of L-carnitine are believed to lower ROS production. Along these lines, ROS have been shown to accelerate the degradation of skeletal muscle proteins, leading to sarcopenia.
L-carnitine-associated dysregulation is also linked to impaired fatty acid utilization, altered glucose homeostasis, and lowered insulin sensitivity. It follows that supplementing with L-carnitine may support metabolism and building muscle.
Accordingly, some data suggest that L-carnitine supplementation can increase muscle protein synthesis. Also, to gain such potential benefits, supplementing with about 2 g of L-carnitine daily is recommended for an average adult.
From potentially enhancing metabolism to possibly improving muscle protein synthesis, which are intertwined physiological processes, L-carnitine may help slow or prevent age-related sarcopenia. Thus, in addition to engaging in an exercise routine, taking L-carnitine supplements may aid older adults’ goals related to preserving physical performance.
Vitamin D
Aside from assuring optimal functioning of major organs like the skin, recent research highlights vitamin D’s crucial role in muscle function. In that regard, vitamin D receptors have been identified on muscle cells. Moreover, vitamin D has been shown to support muscle contraction, strength, and repair.
Also, through its relationship with the gut microbial composition, vitamin D regulates inflammation. Thus, possibly by influencing gut microbes to lower inflammation, getting enough vitamin D could help ensure muscles function optimally during aging.
Despite the importance of vitamin D in overall physiological function, approximately 77% of Americans are considered to have a vitamin D deficiency. As such, vitamin D deficiency is associated with decreased muscle size, impairing muscle strength and functional mobility. This vitamin D deficiency-induced reduction in physical performance can lead to increased risk of sarcopenia and falls.
In contrast to the effects of vitamin D deficiency, vitamin D supplementation has been associated with improved athletic performance. This is the case, especially when vitamin D is taken to target a deficiency of this vitamin.
Hence, vitamin D supplementation may be a way to prevent or slow the occurrence of age-related sarcopenia as people age. Importantly, research-based recommendations suggest taking 10 mcg to 20 mcg of vitamin D daily.
Magnesium
Magnesium is an essential mineral for the regulation of skeletal and heart muscle contraction and relaxation. Moreover, magnesium is required for the synthesis of DNA, RNA, and proteins.
As such, magnesium deficiency is associated with poor physical performance. Also, low circulating magnesium is linked to reduced muscle strength.
On the other hand, supplementation with magnesium may improve skeletal muscle function in older adults. Along those lines, magnesium supplementation has been associated with reduced muscle loss over time.

Recommended doses for aged adults are 320 mg a day for women and 420 mg a day for men. Notably, while supplementation with magnesium may aid in staving off age-related muscle decline, eating plenty of foods that contain magnesium, such as bananas, avocados, spinach, and nuts, can help ensure optimal absorption of this crucial dietary mineral.
Potassium
Another important dietary mineral, potassium, plays a critical role in maintaining cellular function. Dietary intake of potassium, as well as its excretion, maintains a balance of total body potassium content.
As far as dietary potassium intake goes, a transition towards a Westernized diet in different regions of the world has led to a substantial decline in potassium intake compared to traditional diets. As such, a large proportion of the global population is likely experiencing suboptimal potassium intake.
Along these lines, low intake of potassium is linked to reduced insulin sensitivity. Lower insulin sensitivity, in turn, has been tied to muscle protein breakdown and sarcopenia. Furthermore, research in animal models has shown that a diet low in potassium promotes systemic inflammation. Inflammation is a well-known risk factor for muscle loss. Collectively, these findings suggest that high potassium intake may help reduce muscle protein breakdown and lower systemic inflammation.
Accordingly, getting enough potassium to avoid a deficiency may help promote muscle function and physical performance as people age. To get enough potassium, supplementing with potassium bicarbonate, a white solid compound containing potassium, at doses of about 1 g per day may help optimize potassium levels.
Caffeine
Caffeine is a stimulant, consumed by about 80% of people globally. During the day, ATP molecules used for cellular energy are degraded to a compound called adenosine. As such, adenosine accumulates in spaces outside of cells and binds to receptors in the brain called adenosine receptors, causing fatigue and tiredness.
Interestingly, caffeine, a compound structurally similar to adenosine, competes with adenosine to essentially block adenosine receptors. In this way, by preventing adenosine from binding to adenosine receptors, caffeine enhances alertness.
Intriguingly, caffeine can also have other effects, such as increasing muscular endurance and enabling longer workouts. Moreover, according to a cumulative review of studies, caffeine significantly increases muscle strength and endurance.
All the same, caffeine’s effects on physical performance depend on the initial state of arousal for anyone who uses caffeine. In that sense, caffeine can improve physical performance; however, when used at doses that exceed a certain threshold, these benefits decrease. This gets complicated by the observation that dosage thresholds differ from person to person, so figuring out an optimal dose of caffeine for each adult may take practicing trial and error to find how much works best.
Moreover, caffeine intake is associated with mild adverse effects, like anxiety, restlessness, fidgeting, insomnia, irritability, and agitation. These side effects may also increase in magnitude with higher doses of caffeine.
Thus, caffeine may work to enhance older people’s workouts, and some evidence suggests that using caffeine is tied to increased muscle strength. For these reasons, daily consumption of caffeinated beverages, such as coffee, may help ward off skeletal muscle decline and sarcopenia with age.
Deciding Which Supplements to Take to Counteract Age-Related Muscle Decline
A good rule of thumb when picking out supplements to stave off age-related muscle decline is to target a vitamin or mineral deficiency. In that sense, having blood tests done, as administered by a doctor, can help anyone getting older to choose supplements that may help reverse a deficiency. For example, if blood tests show that someone is deficient in magnesium, then supplementing with a compound that promotes higher levels of this mineral may promote better skeletal muscle function.
Furthermore, it may be the case that protein supplementation is one of the most important supplements on the list. In that sense, it is estimated that about 30% of men and 50% of women over age 71 do not get enough protein intake from their diets. Furthermore, inadequate protein intake is a significant contributing factor to sarcopenia in older adults. Thus, in addition to exercising regularly, it is important to get sufficient dietary protein to ward off age-related muscle deterioration.
 Comments
Comments