
Key Points:
- A few studies show that NAD⁺ Drip IV therapy can alleviate alcohol and drug addiction, as well as Parkinson’s disease, but no studies have examined its effects on aging.
- Oral administration of NAD⁺ boosting therapy is safer, more cost effective, and more consistently dosed than intravenous administartion.
NAD⁺ (nicotinamide adenine dinucleotide) IV (intravenous) therapy, also known as NAD⁺ drip therapy, refers to injecting NAD⁺ (dissolved in fluid) into an individual’s vein to raise the concentration of NAD⁺ in the bloodstream to receive the therapeutic benefits of NAD⁺.
Due to the headaches and shortness of breath that some individuals experience with the therapy, IV NAD⁺ is often administered slowly, sometimes measured in drops — hence the term “drip” therapy.
The purpose of NAD⁺ IV therapy is to boost NAD⁺ levels. NAD⁺ is a vital molecule made by our cells to serve hundreds of essential functions. NAD⁺ and its electron-carrying form NADH are required to convert the food we eat into chemical energy.
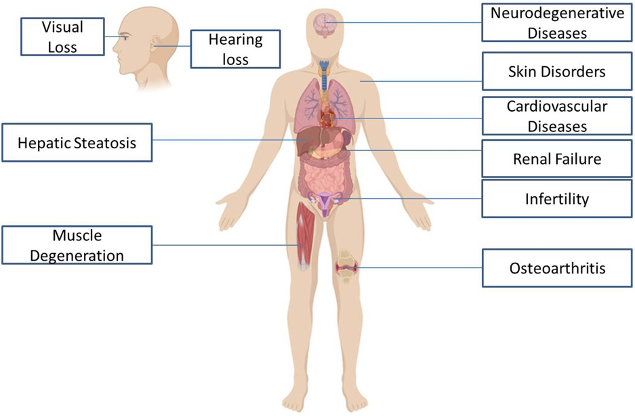
Our NAD⁺ levels tend to decline with age, especially if our diet, sleep, and exercise routines are not optimized. Low NAD+ levels can potentially lead to age-related diseases. Based on mostly animal studies, boosting NAD⁺ can restore NAD⁺ levels, mitigate age-related diseases, and even extend lifespan.
The NAD Drip IV Therapy Research
Alcohol and Drug Addiction
Much of the buzz behind NAD⁺ IV therapy is seemingly based on a couple of research papers published in 1961. In the reports, IV treatment with NAD⁺ (oxidized diphosphopyridine nucleotide) resolved the cravings and withdrawal symptoms of individuals addicted to drugs and alcohol.
Depending on if these individuals experienced headaches and shortness of breath, NAD⁺ infusion ranged from 5 to 35 drops per minute. Even intoxicated patients experienced immediate improvements, and two non-alcoholic individuals who received IV (and intramuscular) NAD⁺ before drinking alcohol had no hangover.
Parkinson’s Disease and Depression
A few studies have shown that NAD⁺ IV therapy alleviates symptoms of Parkinson’s disease, including a case study sponsored by NAD Research Inc. The therapeutic action of NAD⁺ on Parkinson’s disease is associated with the elevation of the neurotransmitter dopamine, essential for movement, which can be uncontrollable in Parkinson’s disease.
Possibly related to raising dopamine levels, a study that tested multiple methods of NADH (reduced from of NAD⁺) administration, including IV, showed that 93% of patients saw improvements in depression, although which of these patients received IV injections was not specified.
Recent Studies
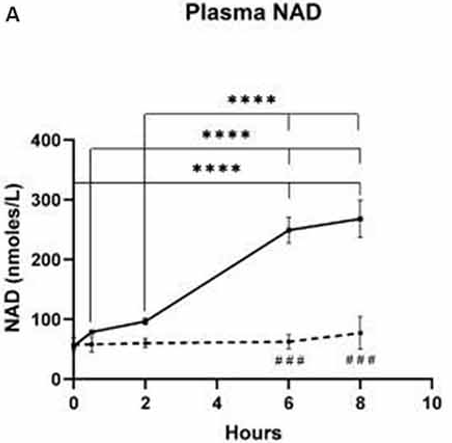
It wasn’t until a 2019 pilot study, sponsored by NAD Research Inc, that bloodstream (plasma) NAD⁺ concentration was measured upon IV NAD⁺ (in normal saline) infusion. The study showed that plasma NAD⁺ did not significantly increase until after 2 hours, suggesting the rapid tissue utilization and metabolism of NAD⁺ within those 2 hours. Dr. David Sinclair, the Harvard scientist who helped repopularize NAD⁺ has mentioned this study on Twitter:
More recently, in another pilot study of 11 male patients between the ages of 35 and 55, NAD⁺ IV therapy improved cognitive function measures. The studies authors include Dr. Susan Broom Gibson, who received consulting fees from NAD⁺ Research Inc., and Dr. Richard Mestayer, a director of NAD⁺ Research Inc. and the Springfield Wellness Center that uses IV NAD⁺ as a clinical therapy. The authors’ state:
“These results combined with case reports in Parkinson’s disease patients suggest that implementation of a standardized cognitive assessment is a practical and effective way to establish efficacy of IV NAD⁺ treatment for clinical conditions involving cognitive impairment.”
Anecdotal Evidence
Although not scientific research, explanations in books support the use of NAD⁺ IV therapy. In his book, NAD Therapy! Too Good to Be True?, psychologist Theo Verwey reveals that he has treated over 6,000 patients with NAD⁺ IV therapy. He hypothesizes that NAD⁺ deficiency is a spectrum disorder manifesting in chronic fatigue, addiction, depression, stress, anxiety, and chronic illness.
Additionally, in her book, Addiction: the Dark Night of the Soul/Nad+: the Light of Hope, therapist Paula Norris Mestayer, wife of Dr. Richard Mestayer and co-founder of NAD⁺ Research Inc. tells the story of her 18 years of working with NAD⁺ IV therapy to help her patients get off alcohol and drugs. In the book, Norris Meystayer says:
“Our nation is in the midst of an opioid epidemic; yet our primary response is to prescribe substitute narcotics, which consign patients to a lifetime on methadone or Suboxone, when there is another, completely natural treatment option available.”
Overall, the clinical research and large volume of anecdotal evidence would suggest that NAD⁺ IV therapy can treat alcohol and drug addiction and Parkinson’s disease. IV NAD⁺ therapy also seems to help with depression and other psychiatric disorders. Still, there now exists multiple options for boosting NAD⁺ levels, and it’s unclear whether intravenously boosting NAD⁺ is the superior method.
Intravenous NAD⁺ vs. Oral NAD⁺
The Real Goal is Boosting NAD⁺
So why isn’t NAD⁺ taken in pill form? This is because when NAD⁺ is administered orally, it metabolizes so quickly that it doesn’t get into the bloodstream. Back in 1961, when used to treat individuals addicted to drugs and alcohol, IV injection was one of the only practical methods for boosting NAD⁺.
Since then, scientists have discovered that NAD⁺ precursors, such as NR (nicotinamide riboside) and NMN (nicotinamide mononucleotide), can be taken orally to boost NAD⁺ levels without any serious short-term side effects.
Irregular IV Administration Cannot Match Consistent Oral Supplementation
With only a few studies testing the effects of IV NAD⁺ on humans or animal models, there are no standard scientifically-backed dosage regimens for IV NAD⁺ therapy. Therefore, the frequency of dosing will vary from clinic to clinic but is usually irregular.
For example, for the anti-aging effects of NAD⁺, a mobile IV service based out of Las Vegas called Reset IV uses three infusions every-other-week followed by monthly maintenance infusions. It is unclear whether this regimen or similar regimens consistently maintain cellular NAD⁺ levels.
In contrast, most of the human and animal model studies testing the effects of oral NAD⁺ precursor supplements, like NR and NMN, use daily supplementation. These studies consistently show a rise in NAD⁺ levels upon supplementation. Thus, daily intake helps to ensure that cellular NAD⁺ levels remain elevated.
IV NAD⁺ Lacks Human Evidence for Anti-Aging Purposes
Of the IV NAD⁺ studies mentioned above, perhaps only the Parkinson’s studies demonstrate any anti-aging effects. Since the age of onset for Parkinson’s patients is around the age of 60, it can be considered an age-related disease.
In comparison, there are now many studies showing that NAD⁺ precursors, particularly NMN have anti-aging benefits, including improving insulin sensitivity, enhancing physical performance and sleep, and increasing muscle strength. Therefore, when it comes to evidence supporting the mitigation of aging in humans, oral NAD⁺ supplementation outperforms IV NAD⁺ therapy.
Is NAD⁺ Drip Better than NAD⁺ Precursor Supplementation?
Until more clinical research is done, it seems unclear which method of administration is better for receiving the benefits of NAD⁺. It may prove unnecessary to receive direct injections. An ideal study would involve comparisons between the clinical outcomes of different NAD⁺ boosting methods.
For example, a study could compare cravings and withdrawal symptoms in individuals with drug and alcohol addiction in response to NAD⁺ IV therapy versus NMN supplementation. Until then, it remains unclear which administration method is better, but it would seem that both should have similar effects.
In a risk-benefit analysis of NAD⁺ therapy, the animal and human research concerning all the methods of boosting NAD⁺ were reviewed. In the review, the authors state that the “literature revolving around IV NAD⁺ is scarce despite its widespread anti-aging marketing.”
However, the lack of studies utilizing IV NAD⁺ administration may be due to research scientists choosing to experiment with NAD⁺ precursors to study the effects of boosting NAD⁺, which is less invasive and not as time-consuming as IV NAD⁺ injection (can take hours). For the same reason, individuals may choose precursors over IV injections.
Body.
Another thing to think about is the costs. The costs of pharmacologically boosting NAD⁺ may vary depending on the location of the NAD⁺ IV therapy clinic or supplement company. However, IV NAD⁺ therapy tends to be more expensive than supplementation. In the end, consumers may choose NAD⁺ precursors out of convenience. Of course, there are natural ways of raising NAD⁺ levels like diet and exercise.
Dosage, Safety, and Regulation
Dosage
Regardless of how NAD⁺ is administered, when it comes to receiving the therapeutic benefits of NAD⁺, it seems that oral supplementation (with precursors) and intravenous injection should have similar results. This of course will depend on the dosage, which depends on what is being treated.
For example, to treat addiction intravenously, a dosage of 300-1000 mg/day of NAD⁺ has been reported. However, since there is limited research on the effects IV NAD⁺ administration on aging, it is difficult to determine the dosage needed to potentially slow aging and prevent age-related disease.
In a case study, a Parkinson’s disease patient was given 500-1500 mg/day of IV NAD⁺ over the course of about eight days and they saw an alleviation of symptoms. In another study, some Parkinson’s disease patients saw symptom improvements after taking 1,000 mg/day of NR for 30 days.
Therefore, the dosage for treating age-related diseases like Parkinson’s disease may be similar between IV NAD⁺ and NAD⁺ precursors like NR, but there is far too little evidence to make this conclusion.
For anti-aging purposes, there are far more studies to suggest the dosage for NAD⁺ precursors. For example, the dosage for NMN seems to be between 500-1000 mg/day, depending on age and weight.
Safety
In general, when it comes to safety, the administration stage of drug intervention is the most prone to error, and intravenous administration results in the most serious medical errors. IV medications have been associated with 56% of medication errors.
If poorly or improperly administered, IV injections can lead to complications such as infection, vein damage, or blood clots. These complications can be avoided by oral administration, which has much less potential for error and harmful outcomes.
Regulation
The administration of intravenous injections is considered a medical practice, thus in most states, businesses that offer IV therapy must be partially owned by a physician. To receive IV therapy, a physician, physician’s assistant, or nurse practitioner must evaluate the individual who is receiving the treatment.
Usually, one of these healthcare practitioners must administer the therapy. A pharmacist or physician can legally compound the drug solution being administered. However, the FDA has become aware of cases where drug compounding does not comply with state regulations.
This can lead to contamination (if not prepared in sterile environment) and poor-quality compounds that can lead to serious illness, or even death. Therefore, if choosing IV NAD⁺ therapy, it is important to find a reputable clinic that follows government regulations.
 Comments
Comments